
When everything was hopeless, Abraham believed anyway, deciding to live not on the basis of what he saw he couldn’t do but on what God said He would do. (Romans 4:18, The Message)
My first appointment with Dr. Mark Weissler, Professor and Chief, Division of Head and Neck Oncology and Surgery at the University of North Carolina School of Medicine took place on Monday, November 21, 2011. This was exactly one week after I learned the protrusion below my right ear, which had increased from roughly the size of a pea to that of a golf ball, in just five weeks, was not an infected gland as I had been led to believe, but instead, a very aggressive cancerous tumor in my right parotid (salivary) gland. These tumors are so rare – occurring in less than one-half of 1 % of the population – that they are often initially misdiagnosed, even by Ear, Nose and Throat doctors. What causes them is unknown.
The appointment was scheduled for 9:30 a.m. Although it takes no longer than thirty-five minutes to get from Raleigh to Chapel Hill on most days, when not traveling during rush hour, we didn’t want to take any chances, so we left with plenty of time to spare. We knew, from past experience, that the major road connecting the two towns (I-40) is often congested and we didn’t want a traffic delay to make the day any more stressful than we anticipated it would be. Once off the highway, we chose a route that was familiar because of its association with our daughter Emily and her years as a student at Carolina. Eventually we would find a quicker way to get from the interstate to the UNC campus, but on this morning it was comforting to drive past Emily’s old dorm and recall the hot August day when we helped her move in her freshman year. It made the approach to the Medical Center feel less intimidating.

The UNC Medical Center
We found our way to Manning Drive, the street on which the North Carolina Memorial Hospital, Women’s Hospital, Children’s Hospital, Neurosciences Hospital and the Cancer Hospital all stand, one impressive building giving way to the next – and all connected indoors by a winding concourse. A parking garage stood across the street, but we weren’t sure which of its several entrances to take. When nothing is familiar it feels a bit like one wrong turn could lead down a rabbit hole, so to speak. But within a matter of weeks, this entire routine – the route to the UNC Medical Center from our home in Raleigh, the entrance to the parking garage (and where we were likely to find a parking space once we were in it) and the walk, hand in hand, across the sky walk (intemperate in winter, because of the wind, but pleasant in summer) from the parking garage to the Cancer Hospital – would become quite familiar, even comforting.

Finally, we reached the E. N. T. clinic where Dr. Weissler sees patients; it is located on the first floor of the Neurosciences Hospital. The waiting room was crowded that morning with adults and children but, after I checked in at the registration desk, Gil and I managed to find two seats together. Every once in a while the door which separates the waiting room from the rooms where patients are seen opened and a nurse standing in the doorway would call out the name of someone waiting to be seen by a doctor. Each time the door opened, we would look up anxiously, but the name called always belonged to someone else. We would then turn back to what we were doing before the door re-opened: trying to read a book, listening to the local news on the flat-screen television hanging on a wall or just starting off into space. We sat in the aptly named “waiting” room for quite a while until finally, the door opened, and my name was called.
The door through which we walked opened onto a warren of hallways, each containing a series of examination rooms. Our first stop was at a nurses’ station where I was weighed and my temperature and blood pressure were taken. Then we were escorted into an examination room to await Dr. Weissler. The first person on his staff to greet us was Sean, his nurse navigator. Sean served as the point of contact between patients with head or neck cancer and the surgeons, oncologists and radiologists who treat them; they all work together as a team. He would prove to be invaluable to us over the coming weeks, getting answers for us quickly whenever we contacted him with questions.
Next, a resident entered the room, introduced himself and began to gather information from me. I gave him the compact disk containing my MRI. He left after examining my neck and head, and said he would return with Dr. Weissler, once they looked at the scan. Although I was anxious, I still had the assumption that removing the tumor would be a simple matter – and that it would be done right away. My E.N.T. doctor in Raleigh had spoken to Gil encouragingly, saying this entire episode would be “just a bump in the road.” But Dr. Weissler quickly dispelled these notions.
He gave us the news in a straightforward, almost blunt manner: the tumor was large and aggressive (which we already knew), and although the MRI indicated that cancer had not progressed beyond the parotid gland, he would have to scrape cancer cells off the nerves, bones and muscles of my face which lie next to the gland. Radiation and chemotherapy would be required as follow-up treatment in an attempt to destroy remaining cancer cells, because he did not think he could get clean margins.
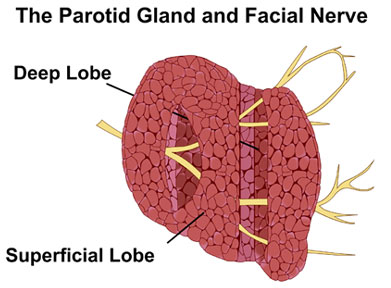
Furthermore, Dr. Weissler did not think it would be possible to remove the parotid gland without also removing a section of the 7th cranial (facial) nerve, which runs through it. Removal of the nerve would result in paralysis on the right side of my face. He also thought removing the tumor might also require removing bone from my jaw and part of the mastoid (from behind my ear). And while he was certain he would need to remove my ear lobe he also thought that it was likely he would not be able to save the skin covering the tumor and that he would need to graft skin and possibly transplant pectoral muscle onto the area to replace any he had to take in order to get all of the tumor. We received this report in stunned silence.
Dr. Weissler paused to see whether we had any questions. Assuming I had heard the worst, I thought for a moment and decided to ask a question designed to elicit a positive response: “So, once the tumor is out, what are my chances of survival?” He answered bluntly, without any hesitation, “Fifty-fifty.” I looked at Gil; we were both speechless. The scenario that was described for us shocked us to the core. I had not considered how difficult it would be to remove the tumor. Disfigurement. It would mean an end to the life I had known for fifty-five years – even if I survived. From now on I would look into the mirror and see a very different face; there would be no way to recover the one I had now. “Is this a future I want for myself?” I thought.
After meeting with Dr. Weissler, we were escorted to the office of the woman who schedules his surgeries and received news that upset us further: the earliest the surgery could be done was December 13 – twenty-two days away. I would have to live with this monster in my body (and it was continuing to grow) for almost another month. But nothing was available sooner. After completing the necessary paperwork, Gil and I made our way back out to the lobby and sat down in the first seats we could find. We could move no further. We sat, motionless, unable to speak to one another, for more than thirty minutes. We did not expect to get this kind of news. This would not be a bump in the road.

This is where we sat.
At some point we managed to get to our feet and look for a cafeteria where we might get something to eat. It would be a while before we could leave the hospital and return to Raleigh. I needed to undergo two C/T scans, one of my chest and one of my thyroid, because Dr. Weissler wanted to rule out any possibility that the tumor had metastasized. Food helped to lift our spirits and I rallied briefly, long enough to complete the tests. But once home, my spirits sank.
That night I kept wondering: If I had gotten a correct diagnosis sooner wouldn’t my chances of survival be much higher? To this question I added another: Why had the Lord let it go undetected for so long? While I knew that this line of questioning would not be helpful, I just couldn’t get past the fact that a more timely diagnosis might have spared both my face and my life. What I needed was a way to get beyond the quagmire of “if only…” It would take a deliberate choice to believe that “God can make a way where no way exists.” I knew that expression well, it’s paraphrase of Romans 4:17 – and I had spoken it to others many times in the past. But now that it was my life that was on the line, I wasn’t sure I could find a way to grab a hold of that promise and hang on to it for dear life. Yet, I knew my life depended on it.
Next week: the Church Militant responds.


“God can make a way where no way exists.” Thank you for sharing your story. You give so much hope and faith in the sharing! We continue to thank God for your healing.
Love, Susan and Russell
Thank you for leaving a comment, Susan. Your words are a blessing to me. Claudia
I am looking forward to being with you next week and continuing to hear your story on this blog. Blessings, Sterling
Thank you, Sterling. See you next week!